In which situations does the squamous cell carcinoma antigen increase? Remember these 13 diseases.
Today, we will explain the tumor marker for squamous cell carcinoma antigen:
What is its essential nature?
What are its functions?
What are its clinical applications?
What is the nature of squamous cell carcinoma antigen?
Squamous Cell Carcinoma Antigen (SCCA) is a glycoprotein with a molecular weight of approximately 48 kDa, which was also discovered thanks to hybridoma technology. In early research, elevated serum SCCA levels were observed in patients with advanced cervical squamous cell carcinoma, laying the groundwork for SCCA as a marker for the diagnosis and prognosis evaluation of squamous cell carcinoma.
SCCA belongs to the superfamily of serine protease inhibitors (SERPINs) and acts as a suicide substrate for cellular proteases. SCCA comprises two highly homologous isoforms—SCCA1 (neutral) and SCCA2 (acidic)—which are encoded by the two genes SERPINB3 and SERPINB4, respectively, located on the long arm of chromosome 18 (18q21.3).
Despite their high homology, SCCA-1 and SCCA-2 have markedly different functions. SCCA1 primarily inhibits papain-like cysteine proteases (including cathepsins L, S, and K) and papain, thereby enhancing the ability of tumor cells to resist programmed cell death, while SCCA2 functions to inhibit chymotrypsin-like serine proteases (including chymase, cathepsin G, etc.), countering inflammation mediated by chymotrypsin-like serine proteases.
Where do both SCCA1 and SCCA2 appear?
SERPINB3 and SERPINB4 are expressed in the squamous cells of tissues including the esophagus, trachea, lung, uterus, prostate, and testis, while SERPINB4 is absent in the thymus and bladder.
In what situations does SCCA increase?
Normal serum SCCA levels are less than 10 μg/L.
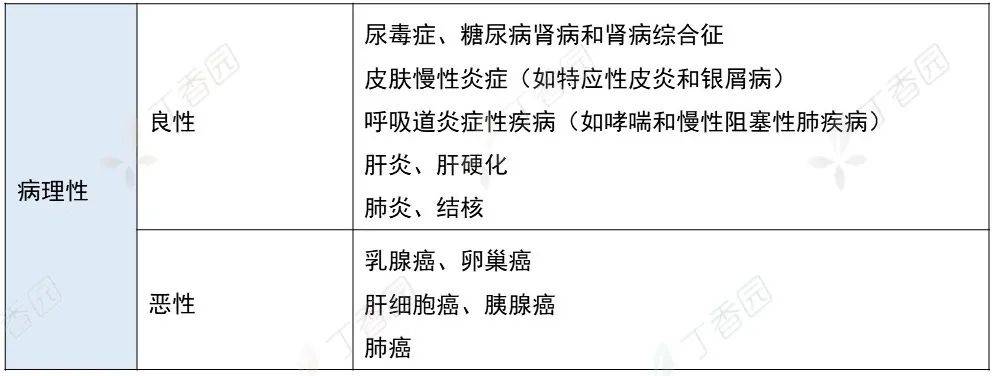
Note: Diseases that cause elevated SCCA in serum include but are not limited to those listed in the table.
1. Cervical cancer
For primary cervical squamous cell carcinoma, the sensitivity is 44% to 69%; for recurrent carcinoma, the sensitivity is 67% to 100%; specificity is 90% to 96%. Its serum level is correlated with tumor development, the extent of invasion into surrounding tissues, and the presence of metastasis. SCCA concentration decreases significantly after radical surgery. SCCA can provide early indication of recurrence; in 50% of patients, elevated SCCA levels precede the clinical diagnosis of recurrence by 2 to 5 months.
2. Lung Squamous Cell Carcinoma: The positive rate varies from 40% to 100%.
Assessing the extent of tumor progression: Its levels are correlated with the extent of tumor progression, with lower positive rates in stages I and II, and higher positive rates in stages III and IV.

Predicting therapeutic efficacy: SCCA helps predict the outcome of lung cancer surgery in the early postoperative period. In patients undergoing radical surgery, the antigen will become negative within 72 hours, while in those receiving palliative resection or exploratory surgery, postoperative SCCA levels remain above normal values.
Monitoring recurrence or metastasis: When postoperative tumor recurrence or metastasis occurs, this antigen rises again before clinical manifestations of recurrence appear. Combined detection with CA125, CYFRA21-1, and CEA can improve diagnostic sensitivity in patients with lung squamous cell carcinoma.
3. Nasopharyngeal Carcinoma
The positive rate increases with disease progression. For advanced-stage patients, its sensitivity can reach 73%, and combined detection of CYFRA21-1 and SCCA can improve the detection sensitivity. The positive rate is 40% in Stage III head and neck cancer and increases to 60% in Stage IV.
4. Esophageal Squamous Cell Carcinoma
Serum SCCA levels are positively correlated with the patient's clinical stage and disease course and can serve as a reference indicator for the auxiliary diagnosis of esophageal cancer and for assessing disease stage and prognosis.
5. Oral Squamous Cell Carcinoma
All show high positive rates, which vary with tumor staging (20%-80%).
Summary:
The sensitivity and specificity of SCCA for auxiliary diagnosis, recurrence monitoring, and prognosis assessment of squamous cell carcinoma are not high. Consider combining SCCA with other tumor markers to improve its sensitivity and specificity.