What exactly are tumor markers, and how do they differ? Have you understood?
With the increase and application of various examination methods, the term tumor markers has become familiar to everyone.
What exactly are tumor markers?
Tumor markers refer to substances that are characteristically present in malignant tumor cells, or abnormally produced by malignant tumor cells, or substances generated by the host in response to tumor stimulation.
They are a class of substances that can reflect tumor occurrence and development, and monitor the response of tumors to treatment. Note: it's a class of substances!

In fact, we all know that there are many types of tumor markers, such as common ones like Alpha-fetoprotein (AFP), Carcinoembryonic Antigen (CEA), CA199, SCC, and so on. Some people may only need to test for two or three types, while others might need to test for over a dozen. What exactly are the differences between these markers?
We generally classify tumor markers into six main types.
I. Carcinoembryonic Antigen Category
Includes alpha-fetoprotein and carcinoembryonic antigen.

1. Alpha-fetoprotein is the most sensitive and specific indicator for diagnosing primary liver cancer, with 80% of liver cancer patients showing elevated levels. Patients with liver diseases generally require regular alpha-fetoprotein testing to prevent the occurrence of liver cancer.
2. Carcinoembryonic antigen is a broad-spectrum tumor marker. Elevated levels may be associated with various cancers, including colorectal cancer, pancreatic cancer, gastric cancer, breast cancer, medullary thyroid carcinoma, liver cancer, lung cancer, ovarian cancer, and urological tumors.
II. Carbohydrate Antigens
In the 1980s, experts utilized hybridoma technology to obtain antibodies capable of recognizing tumor-specific high molecular weight glycoprotein antigens and developed a monoclonal antibody recognition system.

1. CA125 is a specific marker for ovarian cancer. Additionally, CA125 elevation may also be observed in fallopian tube adenocarcinoma, endometrial cancer, cervical cancer, pancreatic cancer, colorectal cancer, breast cancer, and lung cancer.
2. CA50 is a sialic acid ester and sialoglycoprotein, classified as a broad-spectrum tumor marker. Elevations in CA50 can be associated with various malignant tumors, including lung cancer, liver cancer, gastric cancer, ovarian cancer, cervical cancer, cholangiocarcinoma, rectal cancer, and bladder cancer.
3. CA199 is, to date, the marker with the highest sensitivity for pancreatic cancer, with significantly elevated serum CA199 levels observed in most pancreatic cancer patients. Besides pancreatic cancer, other digestive system tumors, as well as ovarian cancer, lymphoma, and breast cancer, can also cause an increase in CA199.
4. CA724 is a laboratory marker used for detecting gastric cancer and various gastrointestinal cancers. It is primarily found in the gastrointestinal tract and exhibits high sensitivity for gastric cancer, ovarian mucinous cystadenocarcinoma, and non-small cell lung cancer. It also shows certain sensitivity for tumors of the biliary system, colorectal cancer, and pancreatic cancer.
5. CA153 is a specific marker for breast cancer, often elevated in breast cancer cases. Its sensitivity is relatively low in the early stages of breast cancer, around 60%, but the positivity rate can reach 80% in metastatic breast cancer. Metastatic ovarian cancer, colon cancer, liver cancer, cholangiocarcinoma, pancreatic cancer, lung cancer, and bronchial cancer can also cause varying degrees of increase in CA153.
6. Squamous cell carcinoma antigen (SCC) is the marker of choice for cervical squamous cell carcinoma. This indicator may also be elevated in some patients with lung cancer, gastric cancer, and ovarian cancer.

7. CA242 is a sialylated glycosphingolipid antigen that is almost always co-expressed with CA50, but the two are recognized by different monoclonal antibodies. CA242 demonstrates higher sensitivity and specificity in the diagnosis of pancreatic cancer, gallbladder cancer, and gastrointestinal cancers.

III. Hormones
Most tumors do not have a fixed relationship with hormones.
1. Human chorionic gonadotropin, abbreviated as HCG, is a glycoprotein secreted by the trophoblast cells of the placenta. It is significant for early pregnancy diagnosis and is also the most sensitive marker for diagnosing trophoblastic cell tumors. Conditions such as seminoma, teratoma, gastric cancer, pancreatic cancer, lung cancer, colon cancer, liver cancer, ovarian cancer, etc., may also cause elevated HCG levels.

2. Catecholamines are a class of substances characterized by the presence of a catechol structure, including epinephrine, norepinephrine, vanillylmandelic acid, and related adrenocortical hormones, which aid in the diagnosis of pheochromocytoma.

IV. Enzymes
Enzymatic tumor markers primarily include PSA, NSE, AFU, and γ-GT.
1. PSA, or prostate-specific antigen, is an antigen related to the prostate. It is secreted and produced by prostate epithelial cells. An elevated PSA level suggests pathological changes or trauma in the prostate. When PSA >10, prostate cancer is suspected.

2. NSE, or neuron-specific enolase, is an acidic protease unique to neurons and neuroendocrine cells. It is a specific marker for neuroendocrine tumors, and conditions such as neuroblastoma, medullary thyroid carcinoma, and small-cell lung cancer can cause an increase in NSE.

3. AFU, or α-L-fucosidase, is a lysosomal acid hydrolase. It shows good sensitivity and a high positive rate in diagnosing hepatocellular carcinoma. When tested simultaneously with alpha-fetoprotein (AFP), it can enhance the detection rate of primary liver cancer.

4. γ-GT, or γ-glutamyl transpeptidase, is widely distributed in human tissues. In normal individuals, serum γ-GT mainly originates from the liver. It is commonly used clinically to diagnose hepatobiliary diseases and is particularly significant for determining whether cancer patients have liver metastases and whether there is recurrence after liver cancer surgery.

5. Protein Class
This primarily refers to cytokeratins and ferritin.
1. Cytokeratin is mainly distributed in epithelial cells and is the primary skeletal protein in keratinocytes, with a total of 20 subtypes. Among them, the degradation of cytokeratin 19 fragment turns into a soluble substance that enters the bloodstream, known as CYFRA21-1. It is the most valuable marker for non-small cell lung cancer, with a sensitivity exceeding 80%.

2. Ferritin, Many malignant tumor cells can synthesize and secrete ferritin, such as hepatocellular carcinoma, lung cancer, pancreatic cancer, leukemia, Hodgkin's disease, multiple myeloma, etc. Ferritin measurement has become one of the auxiliary diagnostic indicators for malignant tumors.

6. Genetic Markers
This includes oncogenes and tumor suppressor genes. Oncogenes can cause malignant cell growth and transformation into cancer, while when tumor suppressor genes mutate and lose or weaken their function, cells can develop into cancer cells.
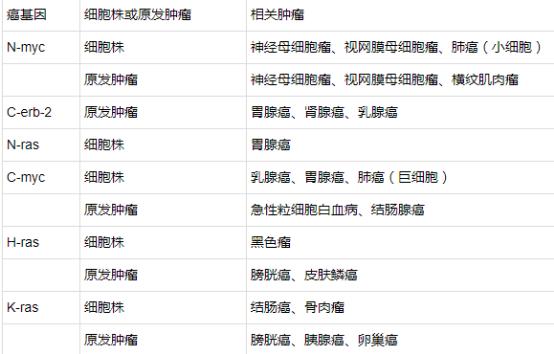
1、Oncogenes include ras genes, myc genes, epidermal growth factor receptors, etc. The following are some common examples.
2. Tumor suppressor genes primarily include two types: RB gene and p53 gene, with the following commonly found examples.

Tumor markers are of significant importance for the diagnosis of malignant tumors, but so far, no ideal tumor marker with 100% specificity and sensitivity has been discovered.
Clinically, there are cases where the diagnosis is confirmed, yet the tumor markers are negative.
Moreover, tumor markers can be influenced by many factors, such as inflammation, improper diet, alcohol consumption, medication, benign tumors, etc., which may all lead to elevated tumor markers.
Therefore, elevated tumor markers do not necessarily indicate malignant tumors, and normal tumor markers do not necessarily rule out malignant tumors.
It's a mouthful, but it's the truth.
The above are only some of the more commonly used tests; some less common or newer testing methods have not been listed, and we welcome any additions.