The "Final Warning" from Gastric Disease to Stomach Cancer: How to Seize the Critical Reversal Period?
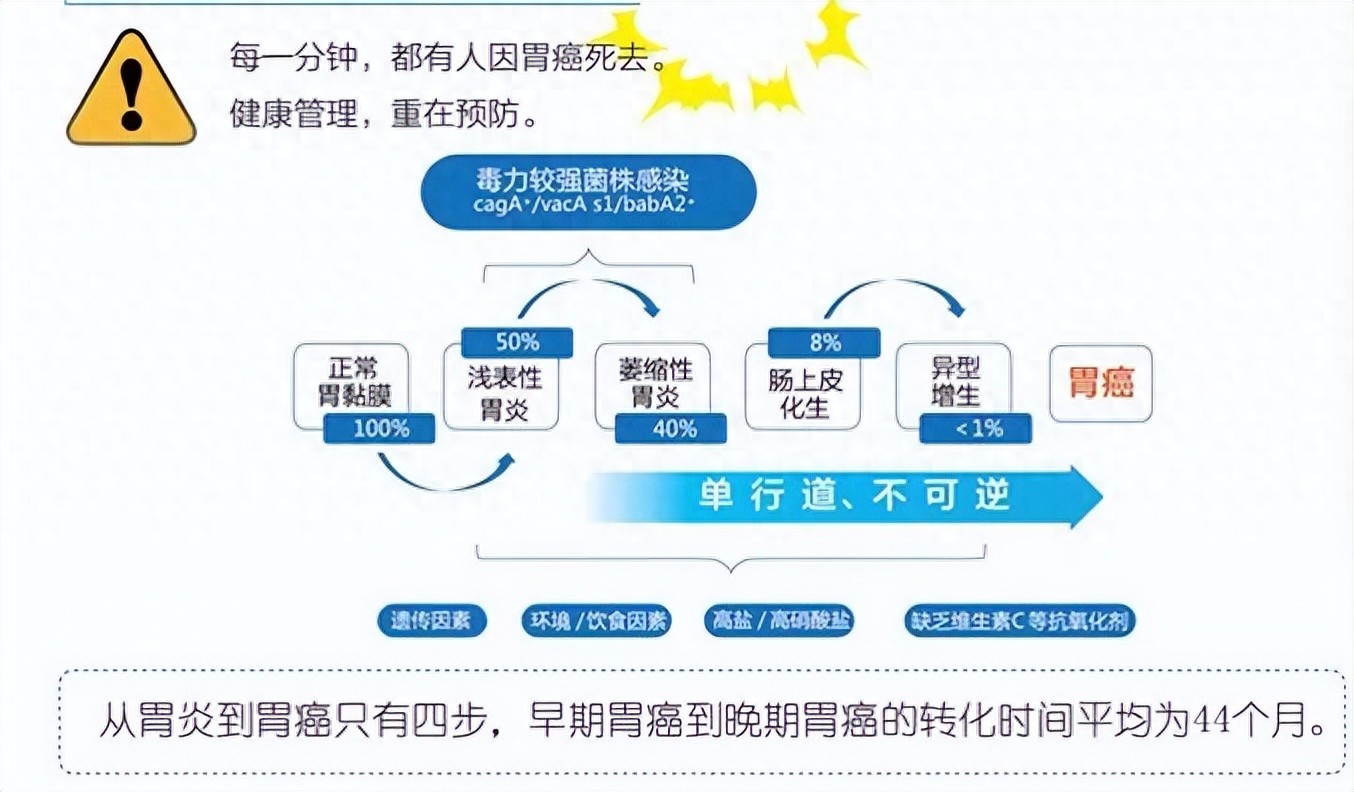
The progression from gastritis to gastric cancer is not instantaneous, but rather a gradual, multi-step process. Among these steps, "intestinal metaplasia" and "dysplasia" are considered the two closest "stepping stones" to gastric cancer, with dysplasia especially regarded as the final warning signal of "precancerous lesions."
Many friends feel very nervous when they see these two terms on their gastroscopy reports. Don't panic—today we'll thoroughly explain: What exactly are they? How high is the risk? And can we successfully intervene before reaching the final stage?
1. What exactly do these two "medical terms" mean?
You can understand it figuratively like this:
Intestinal metaplasia: This can be understood as the stomach mucosa "growing incorrectly" during the repair process after injury. Cells that should have developed into stomach mucosa instead grew to resemble intestinal mucosa. It's like when your home's wall (gastric mucosa) is damaged, but you use your neighbor's (intestine) wallpaper for repairs. This indicates an unstable change has occurred in the gastric environment.
Dysplasia (Intraepithelial Neoplasia): This occurs when new cells not only appear abnormal in structure but also in "quality" – their morphology and arrangement become peculiar, starting to "resemble bad cells." Based on the degree of abnormality, it is classified as low-grade or high-grade.
Low-grade: The cells show a tendency to "go bad," but reversal is still possible.
High-grade: The cells are very close to becoming cancerous, a "red alert" requiring immediate intervention.
II. How High Is the Risk? The Numbers Reveal
Studies indicate that the presence of these lesions significantly increases gastric cancer risk:
Individuals with intestinal metaplasia, especially those with "incomplete intestinal metaplasia," face higher risks.
With low-grade dysplasia, the risk of cancerous transformation is approximately twice as high as in the general population.
With high-grade dysplasia, the risk of cancerous transformation can increase dozens of times, with a significantly higher probability of progressing to cancer within 5 years.
The key point is that this process is modifiable! Our goal is to: halt its progression or even reverse it.
3. Prevention Strategies: A "Counterattack" Roadmap for You
First Foundation: Eradicating the "Culprit" – Helicobacter pylori
As long as the test is positive, regardless of the stage, H. pylori eradication remains the most crucial and effective measure. It can effectively slow or even partially reverse pathological changes and serves as the foundation for all subsequent treatments.
Second Line of Defense: Repairing the "Soil" – Improving Gastric Environment
Control bile reflux: Use prokinetic drugs and mucosal protective agents under medical guidance.
Nutritional supplements: Appropriate supplementation with folic acid, vitamin C, vitamin B12, etc., may aid in mucosal repair, but should be taken under medical supervision.
Consider traditional Chinese medicine: Certain Chinese patent medicines like Morodan have demonstrated potential in improving atrophy and intestinal metaplasia in clinical studies and may serve as adjunctive treatment options.
The Third Decision: Precise "Removal" - Endoscopic Treatment
For focal, clearly defined high-grade intraepithelial neoplasia, waiting is no longer an option. Endoscopic minimally invasive procedures (ESD/EMR) are currently the preferred treatment methods, as they allow complete resection of the lesion for radical cure with minimal trauma and preservation of gastric function.
The Fourth Key: Long-term "Monitoring" - Regular Follow-up Examinations
This is the ultimate safeguard for safety. The frequency of follow-ups depends on the severity of the lesion:
Simple atrophy/intestinal metaplasia: Repeat gastroscopy every 1-3 years.
Low-grade dysplasia: Conduct close follow-up examinations every 6-12 months.
High-grade dysplasia: Requires immediate endoscopic re-examination and evaluation, with treatment typically recommended as soon as possible.
In summary:
Facing intestinal metaplasia and dysplasia, the strategy is to "take it seriously but not panic." Please immediately consult a gastroenterology specialist to develop a personalized plan that includes [Hp eradication + mucosal repair + endoscopic resection when necessary + regular follow-ups]. With proactive intervention, it is entirely possible to eliminate gastric cancer risk in its early stages.
The core views and academic materials in this article were compiled from the WeChat public account "Stomach and Intestine Science Pop" and are published with authorization from the original author. We hereby acknowledge and express our gratitude.